Adhesive capsulitis, commonly known as ‘Frozen Shoulder‘, is characterized by severe pain and stiffness in the shoulder joint leading to restricted Range of Motion (ROM) due to overuse or any injury. However, the range of problems encountering shoulder joints is often misdiagnosed with other conditions. As a result, to treat frozen shoulder effectively, it is mandatory to diagnose the condition carefully.
Objectives:
- Describe frozen shoulder
- Summarize the pathophysiology of frozen shoulder
- Etiology
- Risk factors
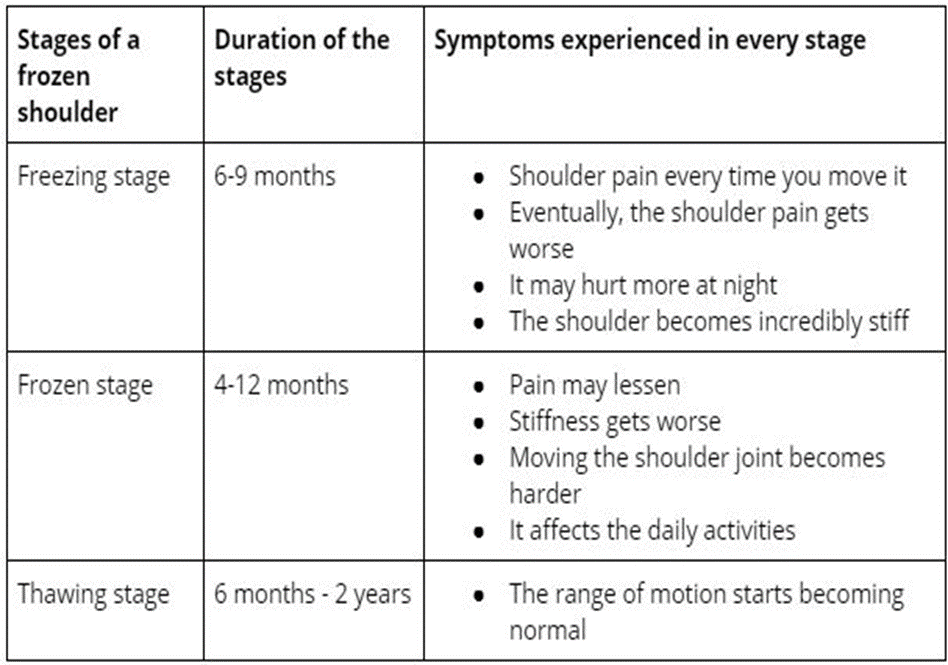
- Clinical stages
- Clinical presentation
- Diagnosis
- Case presentation
- Best sleeping position
- Management
- Medical
- Physical Therapy
- Surgical
Frozen shoulder is a painful condition of the shoulder joint leading to severe pain and stiffness in the joint due to fibrosis of the glenohumeral joint characterized by initially painful later progressively restricted ROM, especially External Rotation. In this condition, the shoulder capsule thickens, becoming tight and stiff, leading to adhesion development. Moreover, Frozen shoulder commonly affects people between 40-60years of age, with females more commonly affected than males. After some time, the symptoms gradually subside; nonetheless, the complete or nearly complete recovery takes almost 2-3years.
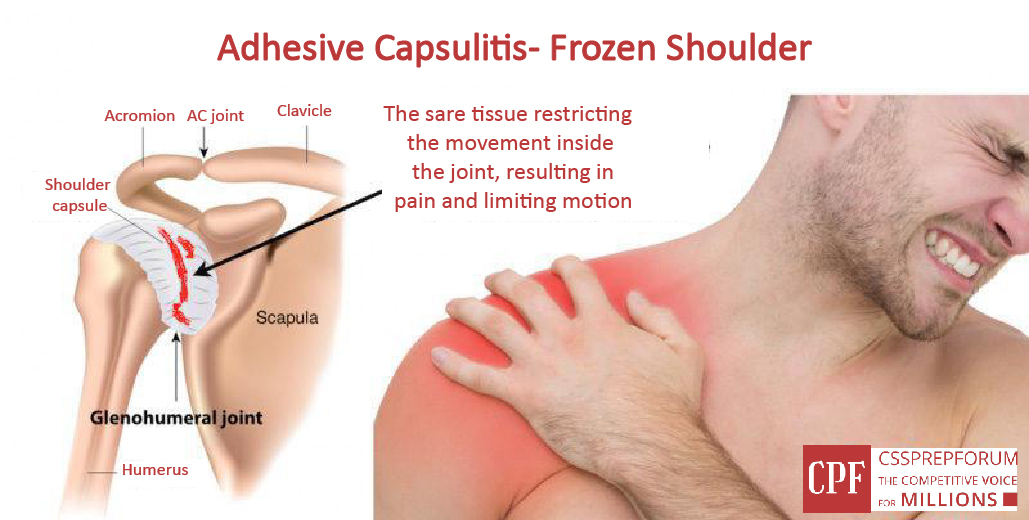
Pathophysiology
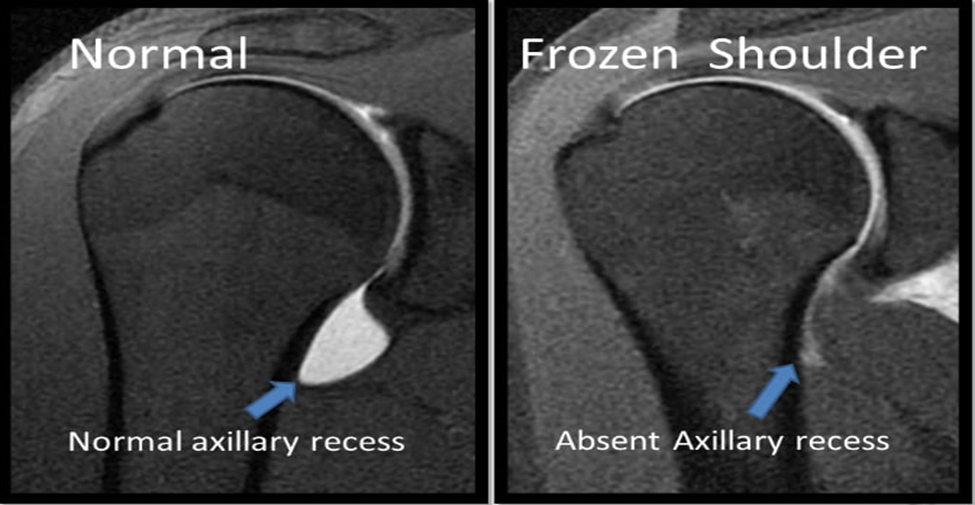
Adhesive capsulitis is often described as the condition caused due to fibrosis and inflammation of the capsule, rotator cuff muscles and ligaments. The structure most commonly affected is coracohumeral ligament limiting External Rotation of the joint. Later, thickening of the glenohumeral joint capsule occurs, limiting ROM in all directions. In addition, patients often suffer from the tight anterior capsule, synovitis, and minor joint with loss of axillary fold. Furthermore, contractures may develop in rotator cuff muscles leading to restricted ROM. In advanced stages, adhesions may develop around the capsule and rotator interval.
Etiology
Primary: Idiopathic (No known cause)
Secondary: Results from a known cause as:
- Systemic: Diabetes Mellitus
- Extrinsic factors: Stroke, Parkinson’s disease, cardiopulmonary disease, humerus fractures.
- Intrinsic factors: Rotator cuff pathology, Bicep tendonitis, Acromioclavicular joint arthritis.
Risk factors
- Diabetes mellitus (most prevalent)
- Stroke
- Thyroid disorder
- Parkinson disease
- Tuberculosis
- Metastatic disease
Clinical presentation
- Insidious onset of diffuse pain in the shoulder joint (dull, aching)
- Pain in the outer shoulder area
- Increase in pain progressively with a gradual decrease in active and passive ROM
- External rotation is most commonly involved
- Movement is limited in multiple planes representing the capsular pattern of the shoulder joint (ER>Abduction>IR)
- Difficulty with ADLs
- Sleep disturbances
- Tightness in the upper trapezius muscle
- The external rotation affects 50% of normal, while Abduction and Internal rotation affect 25% of than normal
Clinical stages
Diagnosis
It is a clinical diagnosis.
Subjective Assessment:
Listen carefully to the patient’s history.
- Distribution of pain and severity: Night pain that aggravates movement. Discomfort lying on the affected side. Pain can be anywhere from the skull base down to the hand.
- History of presenting illness: Aggravating conditions, such as limited reaching, particularly in overhead activities and severe pain while performing ADLs. Complaint of neck pain due to overuse of the cervical muscle.
- Past Medical history: To rule out red flags.
Objective Assessment:
- Observation of posture: Look for the signs of swelling and inflammation. Scapular winging of the affected shoulder may be noticed.
- Palpation: To note any tenderness, muscle spasm, trigger points, or tender points. Point tenderness may be present at the bicipital groove.
- Assessment of ROM (Active, Passive, Overpressure): ROM of Cervical, Thoracic, Shoulder, and rib mobility should be assessed. In frozen shoulder, External rotation is more limited than Abduction, which in turn is more limited than Internal rotation.
- Upper Quarter Exam: To rule out cervical spine involvement, perform UQE.
- Assessment of Glenohumeral and coracohumeral ligamentResisted muscle test: Test for External rotation, Abduction, Internal rotation. Pain at end ROM.
- Assessment of joint accessory movements: Although the anterior and inferior joint capsule is most limited in frozen shoulder, joint mobility will be restricted in all directions.
Special test
Shoulder shrug sign: While performing this test, the patient is unable to lift the affected arm past 90° without elevating the shoulder.
- Hand to neck
- Hand to scapula
- Hand to the opposite scapula

Radiographic evaluation:
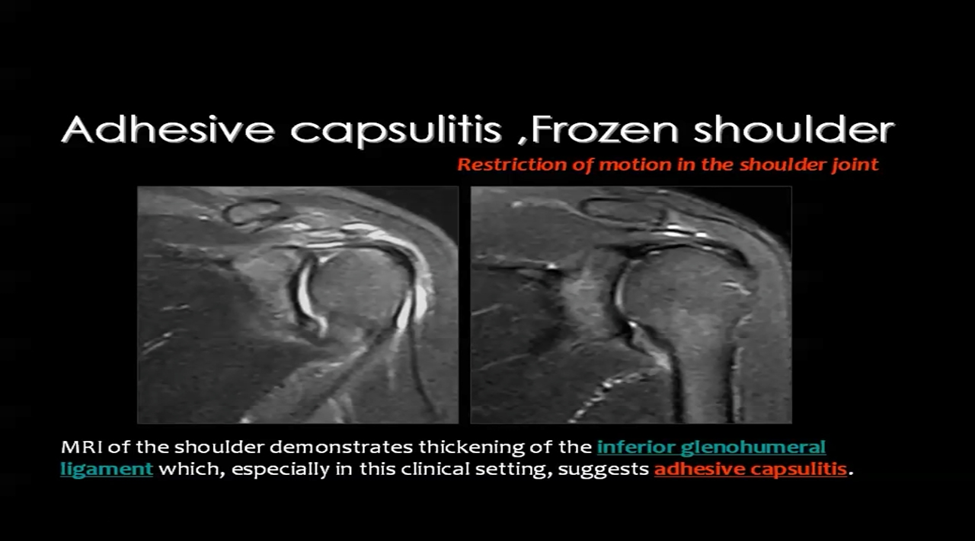
- Magnetic Resonance Imaging: Thickening of coracohumeral ligament and thickening of the joint capsule.
- Arthrography: Standard diagnostic test for frozen shoulder. Reveals 50% reduced volume of involved glenohumeral joint capsule.
Case presentation
Subjective Findings:
Presenting complaint:
A 45year old male patient came with the complaint of left shoulder pain of intensity of 6/10 for a month and restricted left shoulder movements for two weeks.
History of presenting illness:
According to the patient, he was in his usual state of health one month back. After that, he had a fall resulting in an injury to his left shoulder. The injury was trivial, as he slipped and collided with a wall at his left shoulder. After the injury, he had mild pain, which he ignored at first; later, the pain increased in intensity. Initially, the pain was at the end range of motion, but now, it occurs in normal working ROM. Pain increases with activity and reduces with rest. The patient is having difficulty performing ADLs (taking a bath, combing, wearing a shirt). He has taken treatment off and on from his family physician.
Past history:
No, any past medical or surgical history
Family history:
Diabetes and Hypertension
Drug history:
No known drug history
Personal history:
Normal appetite, no recent history of weight loss, sleep disturbance, addicted to cigarette smoking ( one pack a day)
Objective Findings:
Observation and Inspection: On inspection, there was no scar, swelling, or dislocation.
Palpation:
Point tenderness on the bicipital groove and anterior shoulder.
ROM:
External rotation is more limited than Abduction, which in the result is more limited than Internal rotation.
Accessory movements:
Restriction in anterior and inferior gliding movement of left glenohumeral joint.
Neurological testing:
All negative
Management of frozen shoulder
Medical management:
- NSAIDS
- Oral glucocorticoids
- Intra-articular glucocorticoid injection
Physical Therapy Interventions:
Patient education:
- To treat frozen shoulder, patient education is necessary to alleviate frustration and encourage compliance by the patient.
- Educate the patient regarding his condition and duration of treatment.
- Instructions for home exercise program (HEP)
- Avoid painful activities
Sleeping Position:
- Use a cold pack for 15m before going to sleep.
- Use a pillow under your head to keep your body in proper alignment, relaxing your shoulder.
- Consider putting a small cushion under your neck for additional support.
- Try to sleep on the opposite side of the affected shoulder.
- Place a cushion in the armpit area of the affected shoulder.
- People who sleep on their backs all night should use a pillow behind their backs to avoid sudden rolling onto a frozen shoulder arm.

Physical Therapy Treatment for Stage I (Freezing stage)
Treatment goals:
- To reduce pain
- To increase ROM
- To enhance flexibility
- To increase joint range
Treatment options:
- Physical agents: Hot pack
- Electrotherapeutic modalities: TENS, Ultrasound, Laser
- Trigger point release therapy
- Myofascial Release Technique
- Gentle stretching
- Spencer’s Muscle Energy Technique
- Gentle Shoulder Mobilizations
- Pendulum exercises
- Scapular Mobilizations
- Pain management:
- Hot pack: To relieve muscle spasms, use a hot pack for 15m before exercise.

- Electrotherapeutic modalities: To relieve pain and increase ROM, use TENS, Ultrasound and Laser Therapy.
TENS:
- Frequency: 200Hz
- Frequency mode: 20Hz
- Intensity: Patient’s tolerance level
- Duration: 15m for 2times/ week

Therapeutic Ultrasound:
- Decrease pain and increase flexibility.
- Frequency: 1MHz
- Intensity: 1.5watt/cm2
- Duration: 8m continuously in a circular way
- 3days/week for 6weeks

Low-level Laser Therapy:
Strongly suggested for pain and moderately for improving function.
- Device: Ga-Al-As laser
- Wavelength: 810nm
- Power: 60mW
- Duty cycle: 50%
- Spot size: 0.5cm2
- Mode: Continuous
- Energy density: 3.6J/cm2
- Duration: 30s
- Dose/point: 1.8J and Total dose/session: 14.4J
- 12 sessions for 8weeks
High-level Laser Therapy:
- Stimulate joints and muscles more deeply and treat a wider area than LLLT to improve pain and function.
- Wavelength: 1064nm
- Power: 15w
- Duration: 15m
- Separation from the skin: 2.5cm
- Energy density: 100J/cm2
- Duration: Five times per week for three weeks

Trigger point Release Technique:
In the case of frozen shoulder, Trigger points are often found in the Pectoralis major, Bicep tendon, Subscapularis muscle, Deltoid and Trapezius muscle, which add to the severity of pain. Therefore, it is essential to relieving the Trigger points.
- A trigger point in Pectoralis Major:
- A trigger point in Biceps tendon:
- A trigger point in Subscapularis muscle:
- A trigger point in Deltoid muscle:
- A trigger point in the Trapezius muscle:
Myofascial Release Technique ( MFR ):
MFT reduces pain and increases ROM by working on muscles and connective tissue.
- Gentle stretching:
- To increase ROM and decrease stiffness.
- Low-intensity, short duration stretch
- Hold stretch from 1-5s for 5s in a pain-free range, 2-3 times a day.
- A pulley may be used to assist ROM.
• Anterior shoulder stretch:
• Posterior shoulder stretch:
Spencer Technique:
- It is an articulatory technique that utilizes 7 different approaches in which the therapist performs the smooth, passive, rhythmic motion of the shoulder joint to stretch contracted muscles, ligaments and capsules.
- The technique increases pain-free ROM through stretching tissues and increases lymphatic flow and blood circulation.
- Duration: 30m/day, 3times/week for 4 weeks
Gentle Shoulder Mobilizations:
- Low-grade mobilization ( Grade I & II )
- 10-15 repetitions
Anterior mobilization of the humeral head: To increase flexion
Posterior mobilization of humeral head: To increase extension
Inferior/Caudal glide: To increase abduction
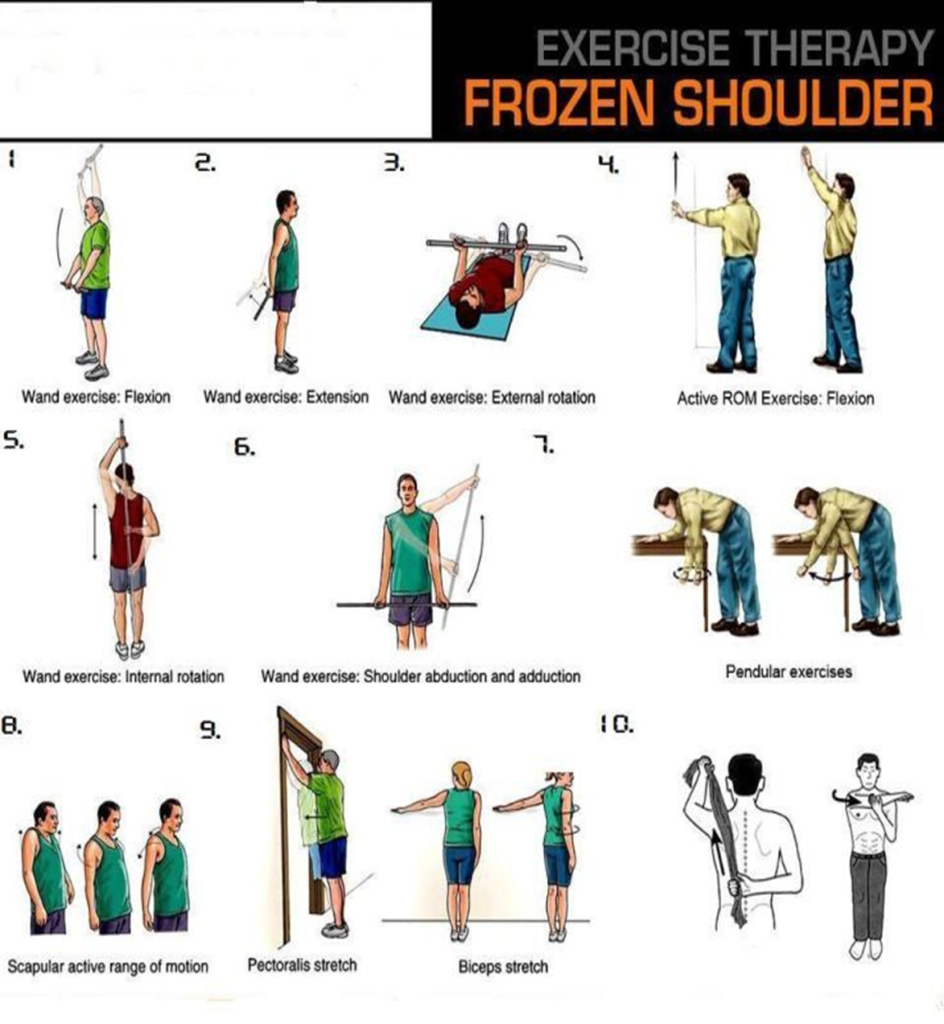
Pendulum exercises:
To mobilize shoulder joint and decrease adhesion formation.
Procedure:
- Stand next to a table about waist thigh
- Place the hand of the unaffected arm on the table for support
- Lean forward slightly without rounding back
- Let the affected arm dangle
- Swing the affected arm in small circles about one foot in width, in one direction for up to 10 revolutions, then reverse to swing arm in the opposite direction for 10 revolutions.
- The diameter of the circle can increase as symptoms improve
- Gradually, this exercise can be made more challenging as the condition improves by holding small weights, about 3-5pounds.
- Scapular Mobilizations:
Together with other exercise program, Scapular Mobilizations aids to reduce soreness, increase ROM and improve scapulohumeral rhythm.
Physical Therapy Treatment for Stage II (Frozen stage)
Treatment goals:
- Increase ROM
- Increase strength
- Regain functional activities
Treatment options:
- Mobilization with Movement
- Aggressive stretching
- End-range Mobilizations
- Shoulder Dyna splint
- Thera band exercises
- Mulligan Technique (Mobilization with Movement):
- It helps to reduce pain, increase end range motion of the shoulder joint by stretching the Glenohumeral joint better than end range mobilizations
- Improves scapulohumeral rhythm
- 3 sets of 20 repetitions with 2m rest in between
- Aggressive stretching:
- To increase ROM
- Low load, prolonged stretch for 10-15s
- Same as that of phase I but increase duration and length of the stretch
- End range Mobilizations:
- Restoration of joint ROM with stretching of peri-articular structures
- 10-15 repetitions
- Low to high grade
- Shoulder Dyna splint (SDS):
Physical Therapy, along with a shoulder Dyna splint, has shown significant improvement in External rotation in patients with frozen shoulders.
- Thera band exercises:
- To increase strength in shoulder musculature, perform Thera band exercises at the shoulder joint
- 5 directions, 3 sets of 12 repetitions, progress with the colour of bands
Physical Therapy Treatment for Stage III ( Thawing stage )
Physiotherapy is most effective in this stage. Increase intensity, frequency and duration of stretch, progress to strengthening exercises program.
Treatment goal:
- Increase strength
- High demand activities
- Back to ADLs
Treatment options:
- Isometric Shoulder Exercises
- Aggressive stretching
- High-grade mobilization ( Grade III & IV ): 3 sets of 30sec
Isometric Shoulder Exercises:
Isometric exercises are helpful for improving physical endurance and posture by strengthening and stabilizing the muscles.
Surgical treatment:
It is considered when conservative treatment fails.
- Arthroscopic capsule release

Who is Dr Sobia Sangrasi?
Dr Sobia Sangrasi is an experienced physiotherapist. Being skilled in her field, she treats patients suffering from the most common movement disorders that hinder their participation in the activities of daily living. To provide the best treatment to her patients and clients, she has indulged herself in evidence-based practice (EBP) to remain updated with the new advances in the treatment protocols. Furthermore, along with a physiotherapist, she is the best counsellor who helps her educate patients regarding the importance of movement and their participation in the treatment. Being a passionate physiotherapist, she prioritizes making people aware of the significance of their posture and movements in day-to-day functioning that, if not considered significant, can lead to a debilitating health condition. Correspondingly, to keep the general public updated, she writes articles about the commonly prevailing conditions and their effective treatment protocol and preventive measures. To get yourself up-to-date regarding the effective treatment of the common conditions faced by your beloved, follow her on social media for recent articles and blogs.